
Bladder cancer is a cancer of the urinary system. A total of 435 new cases were recorded in Hong Kong in 2019, and over 70% of the patients were aged 65 or above.
Due to the high recurrence rate of bladder cancer, early diagnosis and appropriate treatment are very important.
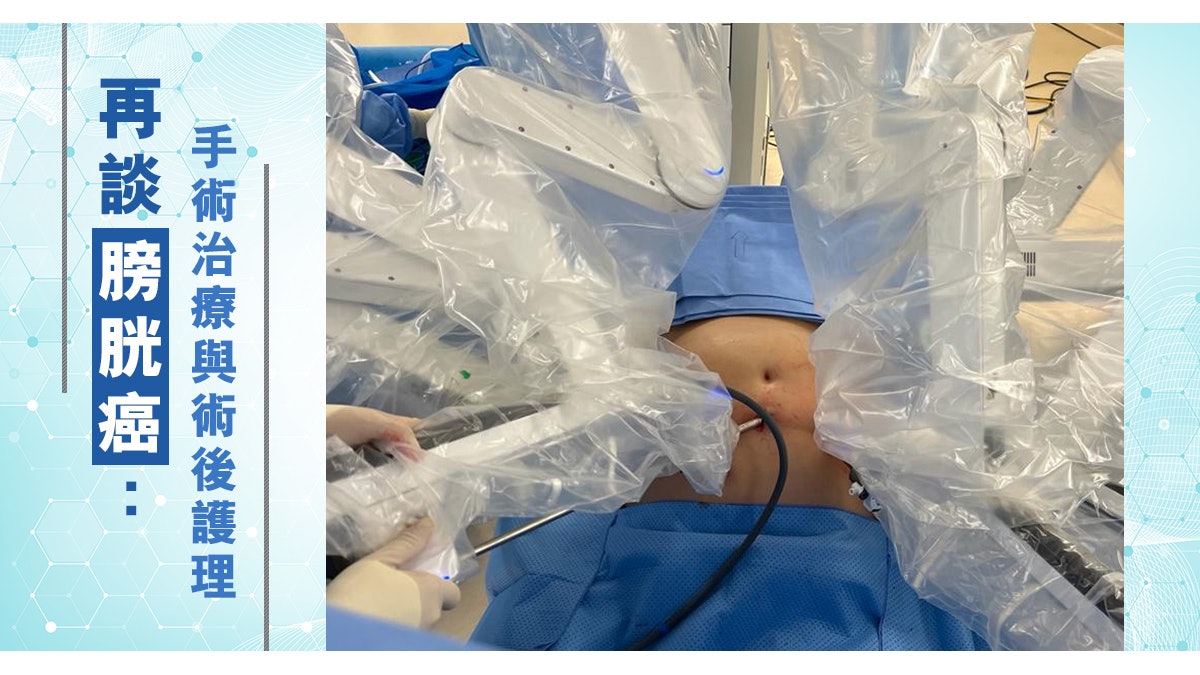
Lin Yaozong, a specialist in urology, said: "Generally speaking, if the tumor has not invaded the bladder muscle layer, the tumor can be removed by endoscopy, the bladder can be preserved, and intra-vesical anticancer drugs can be used after surgery; if the tumor has invaded the bladder muscle layer, the Radical resection of the bladder must be performed, and a stoma or artificial bladder is used to store and urinate after the operation. In recent years, bladder cancer surgery has developed from traditional open to robotic arm-assisted laparoscopy (minimally invasive), with fewer postoperative complications. The recovery time of patients is also greatly shortened.” Dr. Lin Yiu-chung will share the pros and cons of different surgical methods and the matters needing attention in postoperative care below.
The surgical approach depends on the degree of tumor invasion
Bladder cancer can be roughly divided into two categories: "Non-muscle invasive" and "Muscle invasive".
As the name suggests, the former tumor is only confined to the inner wall of the bladder and has not invaded the bladder muscle layer, which belongs to early bladder cancer; the latter refers to cancer cells that have further invaded the muscle layer from the inner wall of the bladder.
The two methods of surgery are very different.
For non-muscle invasive bladder cancer, a "transurethral resection of the bladder tumor" (TURBT) is generally used to remove the tumor tissue and its attached muscle tissue through a cystoscope.
TURBT allows us to assess the type and stage of bladder tumors through tissue tests; for tumors that only invade the superficial bladder, TURBT can achieve the purpose of radical cure.
Postoperative adjuvant therapy includes intravesical chemotherapy, and some patients with a higher risk of recurrence require intravesical Bacillus Calmette-Guérin (BCG) immunotherapy.
The recurrence rate of bladder cancer can be as high as 80% within five years after surgery, and patients must undergo regular postoperative monitoring examinations such as cystoscopy.
Muscle-invasive bladder cancer has the opportunity to spread to other parts of the body because it has penetrated deep into the muscle layer. After diagnosis, full-body imaging scans are needed to check whether the cancer has spread.
If there is no spread, a "radical cystectomy" is usually performed for the patient.
In male patients, the bladder, prostate, seminal vesicles, surrounding lymph glands, and part of the urethra are removed at the same time; in female patients, the bladder, uterus, fallopian tubes, anterior vaginal segment, and lymph glands in the urethra and pelvis are removed at the same time.
Urology specialist Lam Yiu-chung
Pros and cons of enterostomy and artificial bladder
After the bladder is removed, the urinary tract needs to be rerouted so that urine from the ureter can be drained out of the body.
Urinary tract reconstruction methods include the more common "ileostomy" and "in situ ileal bladder" (artificial bladder).
In the former, a 15-centimeter terminal ileum will be cut, connected to the patient's ureter, and a small intestinal stoma will be placed in the right lower abdomen, allowing urine to be discharged through the stoma.
In clinical practice, some patients are often resistant to the stoma for fear of affecting their work and social interactions, and even refuse to undergo surgery for this reason.
If it is assessed to be suitable, an artificial bladder can be considered. The doctor will cut off about 60 cm of the patient's small intestine, make an artificial bladder, place it in the original place of the bladder, and connect the ureters on both sides.
Since the artificial bladder is made of the small intestine, which produces secretions and has no ability to contract on its own and the feeling of urgency to urinate, patients must empty and irrigate the bladder regularly to prevent serious complications caused by inflammation of the artificial bladder.
Although artificial bladder can avoid external stoma, suitable patients must be carefully selected - patients must have good liver and kidney function, their age, self-discipline, long-term self-care ability, and whether they have suitable caregivers, etc., also consider within the range.
At present, the above operations can be performed in a minimally invasive laparoscopic manner assisted by a robotic arm. Several small holes of 5 to 15 mm are used to replace the traditional large open wounds, and the patient's recovery is better.
However, due to the complexity of the operation, it is necessary to cooperate with nursing guidance, physical therapy, occupational therapy and nutritionist follow-up before and after the operation to promote recovery.
In summary, a radical cystectomy is an operation that aims to remove all bladder cancer cells from the body.
The patient needs a preoperative consultation to understand all the procedures involved, and the decision to choose a urinary tract reorganization is a thoughtful one, as the patient adapts to the long-term transition after surgery.
It is true that the need to urinate through a stoma after removal of the bladder may feel uncomfortable or unacceptable at first.
However, most patients are able to over-adapt to a normal life, not only continuing to work but also engaging in various activities, including swimming.
The hospital's professional stoma nursing nurses can guide patients on the use of stoma, daily care and cleaning methods, etc. Some recovered patients serve as volunteers to share their sickness experiences and support fellow travelers in need.
It is hoped that patients can reduce their resistance and concerns about surgery and avoid missing opportunities for treatment.
Urology specialist Lam Yiu-chung
Website of the Hong Kong Society of Urology: https://www.hkua.org
Hong Kong Society of Urology YouTube channel:
https://www.youtube.com/channel/UCUnlbbQ6ugAUSpFY0-g-P7A
(Information provided by the Hong Kong Society of Urology)
*The content of this article is for reference only and does not replace clinical medical advice. If you have any questions, please consult your doctor.






/cloudfront-eu-central-1.images.arcpublishing.com/prisa/2C5HI6YHNFHDLJSBNWHOIAS2AE.jpeg)




